
VITAMIN B
(2011)
EVERYONE WOULD LOVE ME!

Definition
Vitamin A is a fat-soluble vitamin.
Alternative Names
Retinol; Carotenoids
Function
Vitamin A helps form and maintain healthy teeth, skeletal and soft tissue, mucous membranes, and skin. It is also known as retinol because it produces the pigments in the retina of the eye.
Vitamin A promotes good vision, especially in low light. It may also be needed for reproduction and breast-feeding.
Retinol is an active form of vitamin A. It is found in animal liver, whole milk, and some fortified foods.
Carotenoids are dark colored dyes found in plant foods that can turn into a form of vitamin A. One such carotenoid is beta-carotene. Beta-carotene is an antioxidant. Antioxidants protect cells from damage caused by unstable substances called free radicals. Free radicals are believed to contribute to certain chronic diseases and play a role in the degenerative processes seen in aging.
Food SourcesVitamin A comes from animal sources, such as eggs, meat, milk, cheese, cream, liver, kidney, cod, and halibut fish oil. However, all of these sources -- except for skim milk that has been fortified with Vitamin A -- are high in saturated fat and cholesterol.
Sources of beta-carotene are carrots, pumpkin, sweet potatoes, winter squashes, cantaloupe, pink grapefruit, apricots, broccoli, spinach, and most dark green, leafy vegetables. The more intense the color of a fruit or vegetable, the higher the beta-carotene content. These vegetable sources of beta-carotene are free of fat and cholesterol.
Side EffectsIf you don't get enough vitamin A, you are more susceptible to infectious diseases and vision problems.
If you get too much vitamin A, you can become sick. Large doses of vitamin A can also cause birth defects. Acute vitamin A poisoning usually occurs when an adult takes several hundred thousand IU. Symptoms of chronic vitamin A poisoning may occur in adults who regularly take more than 25,000 IU a day. Babies and children are more sensitive and can become sick after taking smaller doses of vitamin A or vitamin A-containing products such as retinol (found in skin creams).
See also: Hypervitaminosis A.
Increased amounts of beta-carotene can turn the color of skin to yellow or orange. The skin color returns to normal once the increased intake of beta-carotene is reduced.
RecommendationsThe best way to get the daily requirement of essential vitamins is to eat a balanced diet that contains a variety of foods from the food guide pyramid.
The Food and Nutrition Board at the Institute of Medicine recommends the following:
Infants
ReferencesHamrick I, Counts SH. Vitamin and mineral supplements. Wellness and Prevention. December 2008:35(4);729-747.
Mason JB. Vitamins, trace minerals, and other micronutrients. In: Goldman L, Ausiello D, eds. Cecil Medicine. 23rd ed. Philadelphia, Pa: Saunders Elsevier; 2007:chap 237.
Anderson RA. Prescribing antioxidants. In: Rakel D, ed. Integrative Medicine. 2nd ed. Philadelphia, Pa: Saunders Elsevier; 2007:chap 103.
Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. National Academy Press, Washington, DC, 2001.
Vitamin A is a fat-soluble vitamin.
Alternative Names
Retinol; Carotenoids
Function
Vitamin A helps form and maintain healthy teeth, skeletal and soft tissue, mucous membranes, and skin. It is also known as retinol because it produces the pigments in the retina of the eye.
Vitamin A promotes good vision, especially in low light. It may also be needed for reproduction and breast-feeding.
Retinol is an active form of vitamin A. It is found in animal liver, whole milk, and some fortified foods.
Carotenoids are dark colored dyes found in plant foods that can turn into a form of vitamin A. One such carotenoid is beta-carotene. Beta-carotene is an antioxidant. Antioxidants protect cells from damage caused by unstable substances called free radicals. Free radicals are believed to contribute to certain chronic diseases and play a role in the degenerative processes seen in aging.
Food SourcesVitamin A comes from animal sources, such as eggs, meat, milk, cheese, cream, liver, kidney, cod, and halibut fish oil. However, all of these sources -- except for skim milk that has been fortified with Vitamin A -- are high in saturated fat and cholesterol.
Sources of beta-carotene are carrots, pumpkin, sweet potatoes, winter squashes, cantaloupe, pink grapefruit, apricots, broccoli, spinach, and most dark green, leafy vegetables. The more intense the color of a fruit or vegetable, the higher the beta-carotene content. These vegetable sources of beta-carotene are free of fat and cholesterol.
Side EffectsIf you don't get enough vitamin A, you are more susceptible to infectious diseases and vision problems.
If you get too much vitamin A, you can become sick. Large doses of vitamin A can also cause birth defects. Acute vitamin A poisoning usually occurs when an adult takes several hundred thousand IU. Symptoms of chronic vitamin A poisoning may occur in adults who regularly take more than 25,000 IU a day. Babies and children are more sensitive and can become sick after taking smaller doses of vitamin A or vitamin A-containing products such as retinol (found in skin creams).
See also: Hypervitaminosis A.
Increased amounts of beta-carotene can turn the color of skin to yellow or orange. The skin color returns to normal once the increased intake of beta-carotene is reduced.
RecommendationsThe best way to get the daily requirement of essential vitamins is to eat a balanced diet that contains a variety of foods from the food guide pyramid.
The Food and Nutrition Board at the Institute of Medicine recommends the following:
Infants
- 0 - 6 months: 400 micrograms per day (mcg/day)
- 7 - 12 months: 500 mcg/day
- 1 - 3 years: 300 mcg/day
- 4 - 8 years: 400 mcg/day
- 9 - 13 years: 600 mcg/day
- Males age 14 and older: 900 mcg/day
- Females age 14 and older: 700 mcg/day
ReferencesHamrick I, Counts SH. Vitamin and mineral supplements. Wellness and Prevention. December 2008:35(4);729-747.
Mason JB. Vitamins, trace minerals, and other micronutrients. In: Goldman L, Ausiello D, eds. Cecil Medicine. 23rd ed. Philadelphia, Pa: Saunders Elsevier; 2007:chap 237.
Anderson RA. Prescribing antioxidants. In: Rakel D, ed. Integrative Medicine. 2nd ed. Philadelphia, Pa: Saunders Elsevier; 2007:chap 103.
Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. National Academy Press, Washington, DC, 2001.
Vitamin A is the name of a group of fat-soluble retinoids, including retinol, retinal, retinoic acid, and retinyl esters [1-3]. Vitamin A is involved in immune function, vision, reproduction, and cellular communication [1,4,5]. Vitamin A is critical for vision as an essential component of rhodopsin, a protein that absorbs light in the retinal receptors, and because it supports the normal differentiation and functioning of the conjunctival membranes and cornea [2-4]. Vitamin A also supports cell growth and differentiation, playing a critical role in the normal formation and maintenance of the heart, lungs, kidneys, and other organs [2].
Two forms of vitamin A are available in the human diet: preformed vitamin A (retinol and its esterified form, retinyl ester) and provitamin A carotenoids [1-5]. Preformed vitamin A is found in foods from animal sources, including dairy products, fish, and meat (especially liver). By far the most important provitamin A carotenoid is beta-carotene; other provitamin A carotenoids are alpha-carotene and beta-cryptoxanthin. The body converts these plant pigments into vitamin A. Both provitamin A and preformed vitamin A must be metabolized intracellularly to retinal and retinoic acid, the active forms of vitamin A, to support the vitamin's important biological functions [2,3]. Other carotenoids found in food, such as lycopene, lutein, and zeaxanthin, are not converted into vitamin A.
The various forms of vitamin A are solubilized into micelles in the intestinal lumen and absorbed by duodenal mucosal cells [5]. Both retinyl esters and provitamin A carotenoids are converted to retinol, which is oxidized to retinal and then to retinoic acid [2]. Most of the body's vitamin A is stored in the liver in the form of retinyl esters.
Retinol and carotenoid levels are typically measured in plasma, and plasma retinol levels are useful for assessing vitamin A inadequacy. However, their value for assessing marginal vitamin A status is limited because they do not decline until vitamin A levels in the liver are almost depleted [3]. Liver vitamin A reserves can be measured indirectly through the relative dose-response test, in which plasma retinol levels are measured before and after the administration of a small amount of vitamin A [5]. A plasma retinol level increase of at least 20% indicates an inadequate vitamin A level [3,5,6]. For clinical practice purposes, plasma retinol levels alone are sufficient for documenting significant deficiency.
A plasma retinol concentration lower than 0.70 micromoles/L (or 20 micrograms [mcg]/dL) reflects vitamin A inadequacy in a population, and concentrations of 0.70–1.05 micromoles/L could be marginal in some people [5]. In some studies, high plasma or serum concentrations of some provitamin A carotenoids have been associated with a lower risk of various health outcomes, but these studies have not definitively demonstrated that this relationship is causal.
Recommended IntakesIntake recommendations for vitamin A and other nutrients are provided in the Dietary Reference Intakes (DRIs) developed by the Food and Nutrition Board (FNB) at the Institute of Medicine of the National Academies (formerly National Academy of Sciences) [5]. DRI is the general term for a set of reference values used for planning and assessing nutrient intakes of healthy people. These values, which vary by age and gender, include:
- Recommended Dietary Allowance (RDA): average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%–98%) healthy individuals.
- Adequate Intake (AI): established when evidence is insufficient to develop an RDA and is set at a level assumed to ensure nutritional adequacy.
- Estimated Average Requirement (EAR): average daily level of intake estimated to meet the requirements of 50% of healthy individuals. It is usually used to assess the adequacy of nutrient intakes in population groups but not individuals.
- Tolerable Upper Intake Level (UL): maximum daily intake unlikely to cause adverse health effects.
Currently, vitamin A is listed on food and supplement labels in international units (IUs) even though nutrition scientists rarely use this measure. Conversion rates between mcg RAE and IU are as follows [7]:
- 1 IU retinol = 0.3 mcg RAE
- 1 IU beta-carotene from dietary supplements = 0.15 mcg RAE
- 1 IU beta-carotene from food = 0.05 mcg RAE
- 1 IU alpha-carotene or beta-cryptoxanthin = 0.025 mcg RAE
Table 1: Recommended Dietary Allowances (RDAs) for Vitamin A [5]AgeMaleFemalePregnancyLactation0–6 months*400 mcg RAE400 mcg RAE 7–12 months*500 mcg RAE500 mcg RAE 1–3 years300 mcg RAE300 mcg RAE 4–8 years400 mcg RAE400 mcg RAE 9–13 years600 mcg RAE600 mcg RAE 14–18 years900 mcg RAE700 mcg RAE750 mcg RAE1,200 mcg RAE19–50 years900 mcg RAE700 mcg RAE770 mcg RAE1,300 mcg RAE51+ years900 mcg RAE700 mcg RAE * Adequate Intake (AI), equivalent to the mean intake of vitamin A in healthy, breastfed infants.
Sources of Vitamin AFood
Concentrations of preformed vitamin A are highest in liver and fish oils [2]. Other sources of preformed vitamin A are milk and eggs, which also include some provitamin A [2]. Most dietary provitamin A comes from leafy green vegetables, orange and yellow vegetables, tomato products, fruits, and some vegetable oils [2]. The top food sources of vitamin A in the U.S. diet include dairy products, liver, fish, and fortified cereals; the top sources of provitamin A include carrots, broccoli, cantaloupe, and squash [4,5].
Table 2 suggests many dietary sources of vitamin A. The foods from animal sources in Table 2 contain primarily preformed vitamin A, the plant-based foods have provitamin A, and the foods with a mixture of ingredients from animals and plants contain both preformed vitamin A and provitamin A.
Table 2: Selected Food Sources of Vitamin A [8]Foodmcg RAE per
servingIU per
servingPercent
DV*Sweet potato, baked in skin, 1 whole1,40328,058561Beef liver, pan fried, 3 ounces6,58222,175444Spinach, frozen, boiled, ½ cup57311,458229Carrots, raw, ½ cup4599,189184Pumpkin pie, commercially prepared, 1 piece4883,743249Cantaloupe, raw, ½ cup1352,70654Peppers, sweet, red, raw, ½ cup1172,33247Mangos, raw, 1 whole1122,24045Black-eyed peas (cowpeas), boiled, 1 cup661,30526Apricots, dried, sulfured, 10 halves631,26125Broccoli, boiled, ½ cup601,20824Ice cream, French vanilla, soft serve, 1 cup2781,01420Cheese, ricotta, part skim, 1 cup26394519Tomato juice, canned, ¾ cup4282116Herring, Atlantic, pickled, 3 ounces21973115Ready-to-eat cereal, fortified with 10% of the DV for vitamin A, ¾–1 cup (more heavily fortified cereals might provide more of the DV)127–14950010Milk, fat-free or skim, with added vitamin A and vitamin D, 1 cup14950010Baked beans, canned, plain or vegetarian, 1 cup132745Egg, hard boiled, 1 large752605Summer squash, all varieties, boiled, ½ cup101914Salmon, sockeye, cooked, 3 ounces591764Yogurt, plain, low fat, 1 cup321162Pistachio nuts, dry roasted, 1 ounce4731Tuna, light, canned in oil, drained solids, 3 ounces20651Chicken, breast meat and skin, roasted, ½ breast5180*DV = Daily Value. DVs were developed by the U.S. Food and Drug Administration (FDA) to help consumers compare the nutrient contents of products within the context of a total diet. The DV for vitamin A is 5,000 IU for adults and children age 4 and older. Foods providing 20% or more of the DV are considered to be high sources of a nutrient. The U.S. Department of Agriculture's (USDA's) Nutrient Database Web site [8] lists the nutrient content of many foods and provides a comprehensive list of foods containing vitamin A in IUs and foods containing beta-carotene in mcg.
Dietary supplements
Vitamin A is available in multivitamins and as a stand-alone supplement, often in the form of retinyl acetate or retinyl palmitate [2]. A portion of the vitamin A in some supplements is in the form of beta-carotene and the remainder is preformed vitamin A; others contain only preformed vitamin A or only beta-carotene. Supplement labels usually indicate the percentage of each form of the vitamin. The amounts of vitamin A in stand-alone supplements range widely [2]. Multivitamin supplements typically contain 2,500–10,000 IU vitamin A, often in the form of both retinol and beta-carotene.
About 28%–37% of the general population uses supplements containing vitamin A [9]. Adults aged 71 years or older and children younger than 9 are more likely than members of other age groups to take supplements containing vitamin A.
Vitamin A Intakes and StatusAccording to an analysis of data from the 2007–2008 National Health and Nutrition Examination Survey (NHANES), the average daily dietary vitamin A intake in Americans aged 2 years and older is 607 mcg RAE [10]. Adult men have slightly higher intakes (649 mcg RAE) than adult women (580 mcg RAE). Although these intakes are lower than the RDAs for individual men and women, these intake levels are considered to be adequate for population groups.
Data from NHANES III, conducted in 1988–1994, found that approximately 26% of the vitamin A in RAEs consumed by men and 34% of that consumed by women in the United States comes from provitamin A carotenoids, with the remainder coming from preformed vitamin A, mostly in the form of retinyl esters [5].
The adequacy of vitamin A intake decreases with age in children [4]. Furthermore, girls and African-American children have a higher risk of consuming less than two-thirds of the vitamin A RDA than other children [4].
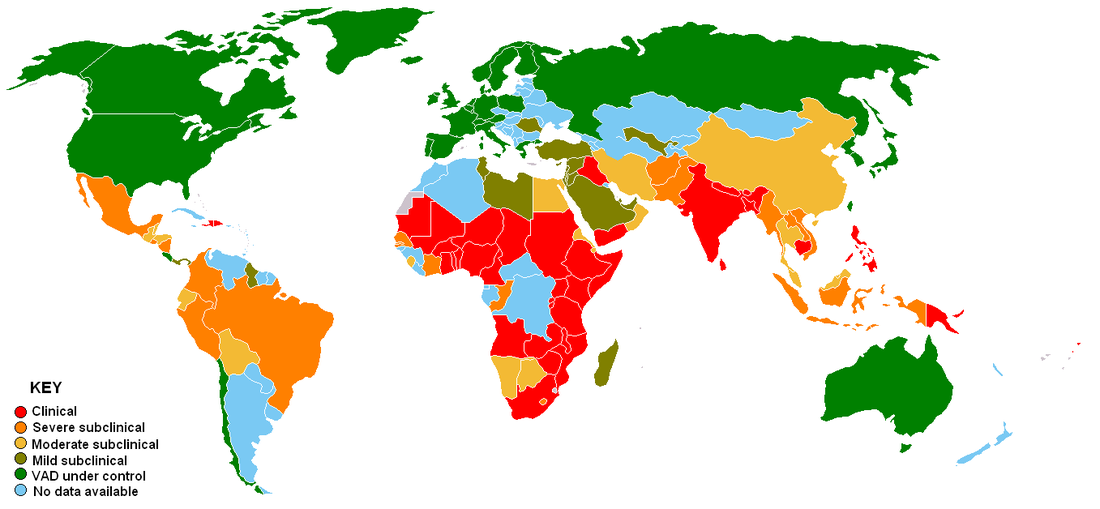
Vitamin A DeficiencyFrank vitamin A deficiency is rare in the United States. However, vitamin A deficiency is common in many developing countries, often because residents have limited access to foods containing preformed vitamin A from animal-based food sources and they do not commonly consume available foods containing beta-carotene due to poverty [2]. According to the World Health Organization, 190 million preschool-aged children and 19.1 million pregnant women around the world have a serum retinol concentration below 0.70 micromoles/L [11]. In these countries, low vitamin A intake is most strongly associated with health consequences during periods of high nutritional demand, such as during infancy, childhood, pregnancy, and lactation.
In developing countries, vitamin A deficiency typically begins during infancy, when infants do not receive adequate supplies of colostrum or breast milk [11]. Chronic diarrhea also leads to excessive loss of vitamin A in young children, and vitamin A deficiency increases the risk of diarrhea [5,12]. The most common symptom of vitamin A deficiency in young children and pregnant women is xerophthalmia. One of the early signs of xerophthalmia is night blindness, or the inability to see in low light or darkness [2,13]. Vitamin A deficiency is one of the top causes of preventable blindness in children [11]. People with vitamin A deficiency (and, often, xerophthalmia with its characteristic Bitot's spots) tend to have low iron status, which can lead to anemia [3,11]. Vitamin A deficiency also increases the severity and mortality risk of infections (particularly diarrhea and measles) even before the onset of xerophthalmia [5,11,13].
Groups at Risk of Vitamin A InadequacyThe following groups are among those most likely to have inadequate intakes of vitamin A.
Premature Infants
In developed countries, clinical vitamin A deficiency is rare in infants and occurs only in those with malabsorption disorders [14]. However, preterm infants do not have adequate liver stores of vitamin A at birth and their plasma concentrations of retinol often remain low throughout the first year of life [14,15]. Preterm infants with vitamin A deficiency have an increased risk of eye, chronic lung, and gastrointestinal diseases [14].
Infants and Young Children in Developing Countries
In developed countries, the amounts of vitamin A in breast milk are sufficient to meet infants' needs for the first 6 months of life. But in women with vitamin A deficiency, breast milk volume and vitamin A content are suboptimal and not sufficient to maintain adequate vitamin A stores in infants who are exclusively breastfed [16]. The prevalence of vitamin A deficiency in developing countries begins to increase in young children just after they stop breastfeeding [3]. The most common and readily recognized symptom of vitamin A deficiency in infants and children is xerophthalmia.
Pregnant and Lactating Women in Developing Countries
Pregnant women need extra vitamin A for fetal growth and tissue maintenance and for supporting their own metabolism [17]. The World Health Organization estimates that 9.8 million pregnant women around the world have xerophthalmia as a result of vitamin A deficiency [11]. Other effects of vitamin A deficiency in pregnant and lactating women include increased maternal and infant morbidity and mortality, increased anemia risk, and slower infant growth and development.
People with Cystic Fibrosis
Most people with cystic fibrosis have pancreatic insufficiency, increasing their risk of vitamin A deficiency due to difficulty absorbing fat [18,19]. Several cross-sectional studies found that 15%–40% of patients with cystic fibrosis have vitamin A deficiency [20]. However, improved pancreatic replacement treatments, better nutrition, and caloric supplements have helped most patients with cystic fibrosis become vitamin A sufficient [19]. Several studies have shown that oral supplementation can correct low serum beta-carotene levels in people with cystic fibrosis, but no controlled studies have examined the effects of vitamin A supplementation on clinical outcomes in patients with cystic fibrosis [19-21].
People with Asthma
People with asthma tend to have low vitamin A serum levels, but it is not clear whether these low levels play a role in asthma causation or are due to the inflammatory process associated with asthma [22-24]. The risk of vitamin A deficiency appears to be higher in children than adults with asthma and is also higher in people with severe disease than those with less severe disease [22]. A study in a rural area of Nepal with chronic vitamin A deficiency showed that vitamin A supplements in pregnant women or their children did not reduce the risk of asthma, wheezing, or spirometric indices of airway obstruction in the children [25]. However, children whose mothers took vitamin A supplements during pregnancy developed higher lung capacity than children whose mothers took a placebo [26].
Vitamin A and HealthThis section focuses on three diseases and disorders in which vitamin A might play a role: cancer, age-related macular degeneration (AMD), and measles.
Cancer
Because of the role vitamin A plays in regulating cell growth and differentiation, several studies have examined the association between vitamin A and various types of cancer. However, the relationship between serum vitamin A levels or vitamin A supplementation and cancer risk is unclear.
Several prospective and retrospective observational studies in current and former smokers, as well as in people who have never smoked, found that higher intakes of carotenoids, fruits and vegetables, or both are associated with a lower risk of lung cancer [1,27]. However, clinical trials have not shown that supplemental beta-carotene and/or vitamin A helps prevent lung cancer. In the Carotene and Retinol Efficacy Trial (CARET), 18,314 current and former smokers (including some males who had been occupationally exposed to asbestos) took daily supplements containing 30 mg beta-carotene and 25,000 IU retinyl palmitate for 4 years, on average [28]. In the Alpha-Tocopherol, Beta-Carotene (ATBC) Cancer Prevention Study, 29,133 male smokers took 50 mg/day alpha-tocopherol, 20 mg/day beta-carotene, 50 mg/day alpha-tocopherol and 20 mg/day beta-carotene, or placebo for 5–8 years [29]. In the beta-carotene component of the Physicians' Health Study, 22,071 male physicians took 325 mg aspirin plus 50 mg beta-carotene, 50 mg beta-carotene plus aspirin placebo, 325 mg aspirin plus beta-carotene placebo, or both placebos every other day for 12 years [30]. In all three of these studies, taking very high doses of beta-carotene, with or without 25,000 IU retinyl palmitate or 325 mg aspirin, did not prevent lung cancer. In fact, both the CARET and ATBC studies showed a significant increase in lung cancer risk among study participants taking beta-carotene supplements or beta-carotene and retinyl palmitate supplements. The Physicians' Health Study did not find an increased lung cancer risk in participants taking beta-carotene supplements, possibly because only 11% of physicians in the study were current or former smokers.
The evidence on the relationship between beta-carotene and prostate cancer is mixed. CARET study participants who took daily supplements of beta-carotene and retinyl palmitate had a 35% lower risk of nonaggressive prostate cancer than men not taking the supplements [31]. However, the ATBC study found that baseline serum beta-carotene and retinol levels and supplemental beta-carotene had no effect on survival [32]. Moreover, men in the highest quintile of baseline serum retinol levels were 20% more likely to develop prostate cancer than men in the lowest quintile [33].
The ATBC and CARET study results suggest that large supplemental doses of beta-carotene with or without retinyl palmitate have detrimental effects in current or former smokers and workers exposed to asbestos. The relevance of these results to people who have never smoked or to the effects of beta-carotene or retinol from food or multivitamins (which typically have modest amounts of beta-carotene) is not known. More research is needed to determine the effects of vitamin A on prostate, lung, and other types of cancer.
Age-Related Macular Degeneration
Age-related macular degeneration (AMD) and cataracts are among the most common causes of significant vision loss in older people. Their etiologies are usually unknown, but the cumulative effects of oxidative stress have been postulated to play a role. If so, nutrients with antioxidant functions, such as provitamin A, might theoretically be used to prevent or treat these conditions.
The Age-Related Eye Disease Study (AREDS), a large randomized clinical trial, revealed that participants with intermediate and advanced AMD could slow the progression of their disease by taking a daily supplement of beta-carotene (15 mg), vitamin E (400 IU dl-alpha-tocopheryl acetate), vitamin C (500 mg), zinc (80 mg), and copper (2 mg) compared with participants taking a placebo [34]. But the researchers did not measure the effects of beta-carotene alone on AMD.
AREDS2, an ongoing multicenter randomized trial in more than 4,000 people aged 50–85 years, will provide a clearer picture of the relationship between carotenoids and AMD [35]. This study is evaluating the effects of supplementation with lutein, zeaxanthin, and omega-3 fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) on advanced AMD progression. The study is also assessing the effects of the original AREDS supplement with less zinc, no beta-carotene, or both on AMD risk.
Measles
Measles is a major cause of morbidity and mortality in children in developing countries. About half of all measles deaths happen in Africa, but the disease is not limited to low-income countries. Vitamin A deficiency is a known risk factor for severe measles. The World Health Organization recommends high oral doses (200,000 IU) of vitamin A for two days for children over age 1 with measles who live in areas with a high prevalence of vitamin A deficiency [36].
A Cochrane review of eight randomized controlled trials of treatment with vitamin A for children with measles found that 200,000 IU of vitamin A on each of two consecutive days reduced mortality from measles in children younger than 2 and mortality due to pneumonia in children [36]. Vitamin A also reduced the incidence of croup but not pneumonia or diarrhea, although the mean duration of fever, pneumonia, and diarrhea was shorter in children who received vitamin A supplements. A meta-analysis of six high-quality randomized controlled trials of measles treatment also found that two doses of 100,000 IU in infants and 200,000 IU in older children significantly reduced measles mortality [37]. The vitamin A doses used in these studies are much higher than the UL. The effectiveness of vitamin A supplementation to treat measles in countries, such as the United States, where vitamin A intakes are usually adequate is uncertain.
The body needs vitamin A to maintain the corneas and other epithelial surfaces, so the lower serum concentrations of vitamin A associated with measles, especially in people with protein-calorie malnutrition, can lead to blindness. None of the studies evaluated in a Cochrane review evaluated blindness as a primary outcome [38]. However, a careful clinical investigation of 130 African children with measles revealed that half of all corneal ulcers in these children, and nearly all bilateral blindness, occurred in those with vitamin A deficiency [39].
Health Risks from Excessive Vitamin ABecause vitamin A is fat soluble, the body stores excess amounts, primarily in the liver, and these levels can accumulate. Although excess preformed vitamin A can have significant toxicity (known as hypervitaminosis A), large amounts of beta-carotene and other provitamin A carotenoids are not associated with major adverse effects [40]. The manifestations of hypervitaminosis A depend on the size and rapidity of the excess intake. The symptoms of hypervitaminosis A following sudden, massive intakes of vitamin A, as with Arctic explorers who ate polar bear liver, are acute [41]. Chronic intakes of excess vitamin A lead to increased intracranial pressure (pseudotumor cerebri), dizziness, nausea, headaches, skin irritation, pain in joints and bones, coma, and even death [2,4,5]. Although hypervitaminosis A can be due to excessive dietary intakes, the condition is usually a result of consuming too much preformed vitamin A from supplements or therapeutic retinoids [3,5]. When people consume too much vitamin A, their tissue levels take a long time to fall after they discontinue their intake, and the resulting liver damage is not always reversible.
Observational studies have suggested an association between high intakes of preformed vitamin A (more than 1,500 mcg daily—only slightly higher than the RDA), reduced bone mineral density, and increased fracture risk [1,4,42]. However, the results of studies on this risk have been mixed, so the safe retinol intake level for this association is unknown.
Total intakes of preformed vitamin A that exceed the UL and some synthetic retinoids used as topical therapies (such as isotretinoin and etretinate) can cause congenital birth defects [2-4]. These birth defects can include malformations of the eye, skull, lungs, and heart [4]. Women who might be pregnant should not take high doses of vitamin A supplements [2].
Unlike preformed vitamin A, beta-carotene is not known to be teratogenic or lead to reproductive toxicity [1]. And even large supplemental doses (20–30 mg/day) of beta-carotene or diets with high levels of carotenoid-rich food for long periods are not associated with toxicity. The most significant effect of long-term, excess beta-carotene is carotenodermia, a harmless condition in which the skin becomes yellow-orange [1,27]. This condition can be reversed by discontinuing beta-carotene ingestion.
Supplementation with beta-carotene, with or without retinyl palmitate, for 5–8 years has been associated with an increased risk of lung cancer and cardiovascular disease in current and former male and female smokers and in male current and former smokers occupationally exposed to asbestos [29,43]. In the ATBC study, beta-carotene supplements (20 mg daily) were also associated with increased mortality, mainly due to lung cancer and ischemic heart disease [29]. The CARET study ended early, after the investigators found that daily beta-carotene (30 mg) and retinyl palmitate (25,000 IU) supplements increased the risk of lung cancer and cardiovascular disease mortality [43].
The FNB has established ULs for preformed vitamin A that apply to both food and supplement intakes [5]. The FNB based these ULs on the amounts associated with an increased risk of liver abnormalities in men and women, teratogenic effects, and a range of toxic effects in infants and children. The FNB also considered levels of preformed vitamin A associated with decreased bone mineral density, but did not use these data as the basis for its ULs because the evidence was conflicting. The FNB has not established ULs for beta-carotene and other provitamin A carotenoids [27]. The FNB advises against beta-carotene supplements for the general population, except as a provitamin A source to prevent vitamin A deficiency.
Table 3: Tolerable Upper Intake Levels (ULs) for Preformed Vitamin A [5]*AgeMaleFemalePregnancyLactation0–12 months600 mcg RAE
(2,000 IU)600 mcg RAE
(2,000 IU) 1–3 years600 mcg RAE
(2,000 IU)600 mcg RAE
(2,000 IU) 4–8 years900 mcg RAE
(3,000 IU)900 mcg RAE
(3,000 IU) 9–13 years1,700 mcg RAE
(5,667 IU)1,700 mcg RAE
(5,667 IU) 14–18 years2,800 mcg RAE
(9,333 IU)2,800 mcg RAE
(9,333 IU)2,800 mcg RAE
(9,333 IU)2,800 mcg RAE
(9,333 IU)19+ years3,000 mcg RAE
(10,000 IU)3,000 mcg RAE
(10,000 IU)3,000 mcg RAE
(10,000 IU)3,000 mcg RAE
(10,000 IU)* These ULs, expressed in mcg and in IUs (where 1 mcg = 3.33 IU), only apply to products from animal sources and supplements whose vitamin A comes entirely from retinol or ester forms, such as retinyl palmitate. However, many dietary supplements (such as multivitamins) do not provide all of their vitamin A as retinol or its ester forms. For example, the vitamin A in some supplements consists partly or entirely of beta-carotene or other provitamin A carotenoids. In such cases, the percentage of retinol or retinyl ester in the supplement should be used to determine whether an individual's vitamin A intake exceeds the UL. For example, a supplement labeled as containing 10,000 IU of vitamin A with 60% from beta-carotene (and therefore 40% from retinol or retinyl ester) provides 4,000 IU of preformed vitamin A. That amount is above the UL for children from birth to 13 years but below the UL for adolescents and adults.
Interactions with MedicationsVitamin A can interact with certain medications, and some medications can have an adverse effect on vitamin A levels. A few examples are provided below. Individuals taking these and other medications on a regular basis should discuss their vitamin A status with their health care providers.
Orlistat
Orlistat (Alli®, Xenical®), a weight-loss treatment, can decrease the absorption of vitamin A, other fat-soluble vitamins, and beta-carotene, causing low plasma levels in some patients [44]. The manufacturers of Alli and Xenical recommend encouraging patients on orlistat to take a multivitamin supplement containing vitamin A and beta-carotene, as well as other fat-soluble vitamins [45,46].
Retinoids
Several synthetic retinoids derived from vitamin A are used orally as prescription medicines. Examples include the psoriasis treatment acitretin (Soriatane®) and bexarotene (Targretin®), used to treat the skin effects of T-cell lymphoma. Retinoids can increase the risk of hypervitaminosis A when taken in combination with vitamin A supplements [44].
Vitamin A and Healthful DietsThe federal government's 2010 Dietary Guidelines for Americans notes that "nutrients should come primarily from foods. Foods in nutrient-dense, mostly intact forms contain not only the essential vitamins and minerals that are often contained in nutrient supplements, but also dietary fiber and other naturally occurring substances that may have positive health effects. ...Dietary supplements...may be advantageous in specific situations to increase intake of a specific vitamin or mineral."
The Dietary Guidelines for Americans describes a healthy diet as one that:
- Emphasizes a variety of fruits, vegetables, whole grains, and fat-free or low-fat milk and milk products.Many fruits, vegetables, and dairy products are good sources of vitamin A. Some ready-to-eat breakfast cereals are fortified with vitamin A.
- Includes lean meats, poultry, seafood, beans and peas, eggs, and nuts and seeds.Beef liver contains high amounts of vitamin A. Other sources of the nutrient include some fish, beans, and nuts.
- Limits solid fats (saturated fats and trans fats), cholesterol, salt (sodium), added sugars, and refined grains.
- Stays within your calorie needs.

|
Vitamin A deficiency (avitaminosis A) remains endemic in large areas of the world and continues to be a major cause of visual disability and mortality. Estimates predict that more than five million children develop xerophthalmia annually and that a quarter million or more become blind from the effects of vitamin A deficiency. It is also a major pathway for measles-associated blindness, particularly in Africa. In most developed countries the vitamin A requirements are satisfactorily met, but cases of deficiency sometimes occur, especially in newborns and pregnant and nursing women, whose nutritional needs are greatest. Vitamin A deficiency can result from an inadequate intake, faulty absorption (as in sprue, celiac disease, cystic fibrosis and other conditions causing steatorrhea) and less often with defective storage (as in liver disease). Healthy humans on a diet deficient in vitamin A and carotenoidsdevelop evidence of the deficiency after time periods ranging from a few weeks to about a year. Manifestations of vitamin A deficiency include cessation of growth, night blindness, and an increased susceptibility to infection. Epidemiological studies have shown an inverse relationship between cancer risk and vitamin A consumption and much has been written about retinoids and neoplasms and about the ability of retinoids to modify cellular differentiation and proliferation. The levels of retinol, retinol-binding protein and transthyretinin the blood are directly related. If malnourished children, who are deficient in vitamin A, are given vitamin A parentally the serum retinol-binding protein does not increase for 24 hours. On the other hand, when protein and vitamin A are given to children with kwashiorkor or marasmusthe serum levels of retinol-binding protein, transthyretin and vitamin A all increase . These observations point to an impaired hepatic release of vitamin A rather than to an actual vitamin A deficiency. Rats deprived of vitamin A, but fedretinoic acid become blind and sterile but otherwise appear healthy. Evidently retinol or retinalfunction in vision and reproduction whereas the maintenance of mucous secretions and some functions of vitamin A only requires retinoic acid. Giving retinoic acid to rats on a diet deficient in vitamin A and in carotenoids prevents all the signs of vitamin A deficiency, including the external ocular changes, except night blindness.
|